
Medical Oxygen Needs Tracker
An interactive tool to help advocates, decision-makers, and implementers communicate the importance of investing in access to medical oxygen as a critical component of health systems in low- and middle-income countries.
Note: For the best viewing experience, this dashboard is designed for use on a PC or monitor. Mobile devices may not provide an optimal display.
About this resource
Oxygen is a lifesaving medicine with no substitute—essential across ages, countries, and health conditions, including COVID-19, severe pneumonia, newborn conditions, and obstetric emergencies. Yet equitable access to medical oxygen, paired with pulse oximetry, remains inadequate across many health facilities in low- and middle-income countries. Fewer than one in three people in these countries who need oxygen for acute medical or surgical conditions receive it due to gaps in service contact, readiness, provision, and quality. As we work to advance progress for universal health coverage and other targets for the Sustainable Development Goals, putting strong national medical oxygen systems at the forefront of global health is critical.
About the tool: The Medical Oxygen Needs Tracker is an advocacy tool intended to help elevate the importance of investing in access to reliable oxygen delivery systems to meet the needs of all related health conditions and populations in low- and middle-income countries. The tracker estimates the daily volume of medical oxygen needed to treat all inpatients with acute hypoxemia (a sudden decrease in oxygen levels in the blood) in a number of health conditions and the existing treatment gaps across these countries; it does not cover long-term medical oxygen need for chronic hypoxemia or medical oxygen need for surgeries. As such, it is not intended to be used for planning or procurement purposes.
For COVID-19-specific oxygen need estimates, see our COVID-19 Oxygen Needs Tracker.
How to use the tool:
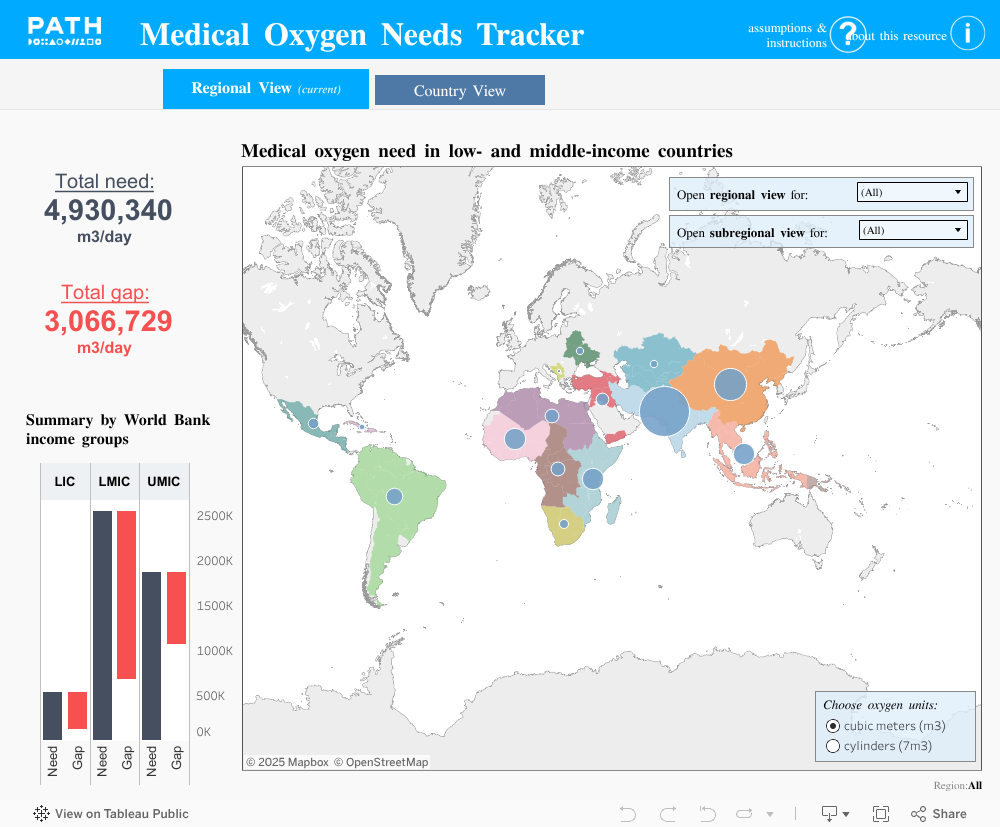
Users can filter the dashboard by region (Africa, Asia, Europe, Latin America and the Caribbean, and Oceania) or further by subregion; switch between oxygen units of volume (cubic meters or cylinders); and toggle between geographic levels (regional or country view) in the map visualization. Regional and subregional classifications in the dashboard are from the United Nations Statistical Division.
The numbers to the left highlight the total daily medical oxygen need and the gap in high-quality oxygen coverage for acute hypoxemia.
The bar chart displays the total daily medical oxygen need and coverage gap across low- and middle-income countries. It aggregates the data according to World Bank income groups (low-income/LIC, lower-middle-income/LMIC, and upper-middle-income/UMIC). Hovering over each bar showcases total oxygen need (black), total oxygen gap (red), and total existing oxygen capacity (white) for the specific region or subregion selected (or all low- and middle-income countries as default).
The map is visualized according to oxygen need, corresponding to the size of the bubble. A tooltip appears when hovering over each bubble and provides descriptive summaries of oxygen need and oxygen gap (if ‘regional view’ is selected).
Assumptions:
A model to estimate the volume of medical oxygen needed in low- and middle-income countries to treat acute hypoxemia for various health conditions and the current gaps in high-quality medical oxygen treatment was developed by PATH.
Data from the Global Burden of Disease (GBD) study (2021) by the Institute for Health Metrics and Evaluation (IHME) were used as an input to capture country-level annual disease burden; that disease burden was forecasted to present times, assuming trends from 2014 to 2021 are maintained. In this tool, inpatients presenting with the acute need for medical oxygen are considered, based on a list of 21 conditions outlined in the report from the Lancet Global Health Commission on medical oxygen security. COVID-19 disease burden was forecasted differently, using annual hospitalization rate estimates from the US Centers for Disease Control and Prevention and UN population projections, given that historical trends do not reflect current disease patterns.
Existing literature, expert opinion, and other data sources informed assumptions about oxygen needs and delivery gaps, including:
- The set of health conditions requiring an acute need for medical oxygen support (The Lancet Global Health Commission).
- The proportion of annual cases, by condition and age category, that require hospitalization (The Lancet Global Health Commission).
- Hypoxemia prevalence, by region, age category, and condition, to estimate hypoxemia cases (The Lancet Global Health Commission).
- Treatment assumptions (flow rates and treatment duration) to estimate age- and condition-specific oxygen volume needed (unpublished longitudinal study of hypoxemia prevalence and oxygen consumption by PATH).
- Country-specific predictions of the oxygen need met by existing oxygen delivery capacity using regional gap estimates (The Lancet Global Health Commission), country burden of lower respiratory infections (IHME GBD), health spend (World Bank), and expert judgements of oxygen access.
As these estimates reflect only medical oxygen need and quality coverage gaps for patients with acute hypoxemia, the tracker likely underestimates the total oxygen need for a country or region. Data gaps regarding hospitalization rates and hypoxemia prevalence for certain conditions, age groups, and geographies, as well as oxygen coverage within a country, may also impact these estimates.
This tracker DOES NOT account for unanticipated disease patterns, (e.g., outbreaks, climate-driven changes), changes due to recent health campaigns (e.g., vaccination or prevention campaigns), or recent changes in oxygen treatment coverage (e.g., increases or decreases in oxygen delivery infrastructure due to investment, policy change, conflict, or natural disaster).
Acknowledgement: This resource was developed as part of the Strengthening Oxygen Utilization and Respiratory Care Ecosystems (SOURCE) project led by PATH and funded by the Gates Foundation.
Photo: PATH/Janet Shauri.


