
This is the third article in our series exploring what the foreign assistance funding gaps could mean for women and children around the world. Read the first article here and the second article here.
Pregnancy, the transition to motherhood, and the first month of life should be periods of joy and celebration. Yet, for many women and babies, these life-giving experiences often come with life-threatening challenges that are completely preventable.
Every two minutes, a woman dies from complications in pregnancy and childbirth, seven babies are stillborn, and eight newborns die within their first 28 days of life.
The vast majority of maternal deaths—92 percent—happen in low- and lower-middle-income countries. In fact, in low-income countries, women and girls face a 1 in 66 chance of dying due to maternal causes in their lifetime—a shocking figure, when that same lifetime risk for women and girls in high-income countries is only 1 in nearly 8,000.

Data source: WHO fact sheet on maternal mortality, updated April 2025.
The good news is that global investments in making pregnancy and childbirth safer have led to remarkable progress. These investments have expanded access to care before, during, and after birth; helped prevent and treat common, but dangerous complications like high blood pressure or bleeding; and provided important medicines when needed.
Since 2000, maternal mortality has dropped by 40 percent worldwide. And in 2023, for the first time ever, not a single country was recorded as facing extremely high maternal mortality by the World Health Organization (WHO). Healthier moms and safer pregnancies and deliveries also mean healthier babies. Stillbirths and neonatal deaths have similarly improved since 2000, dropping 37 percent and 44 percent, respectively.
As donor countries shrink their investments in global health assistance, this hard-won progress for mothers and newborn babies is under threat, especially for those already facing the highest risks.
Global financing for maternal health
Continuing our deep dive into financing data from the Institute for Health Metrics and Evaluation (IHME), we analyzed the amount of development assistance for health (DAH) global donors provided for maternal health.* In 2022, $5.05 billion of global DAH was mobilized for maternal health. This funding came from a broad and evenly spread coalition of donors, with more than $1 billion contributed by private donors alone.
Nearly $4 in every $10 of DAH for maternal health was funneled from donors to recipients through multilateral United Nations (UN) agencies. Unfortunately, all seven leading government donors, which account for nearly half of all maternal health DAH, have announced cuts to their foreign assistance budgets in 2025 and the years ahead. While the specific cuts to be made by some major global donors like the UK aren’t yet known, multilateral organizations, such as those facilitated by the UN, are likely to be a common target. Germany, the US, and the Netherlands have already announced plans to reduce funding for some of the global institutions that support maternal and newborn health. It’s clear this channel for investment will continue to shrink, and the risk of losing decades of progress in ending preventable maternal and newborn deaths will grow.
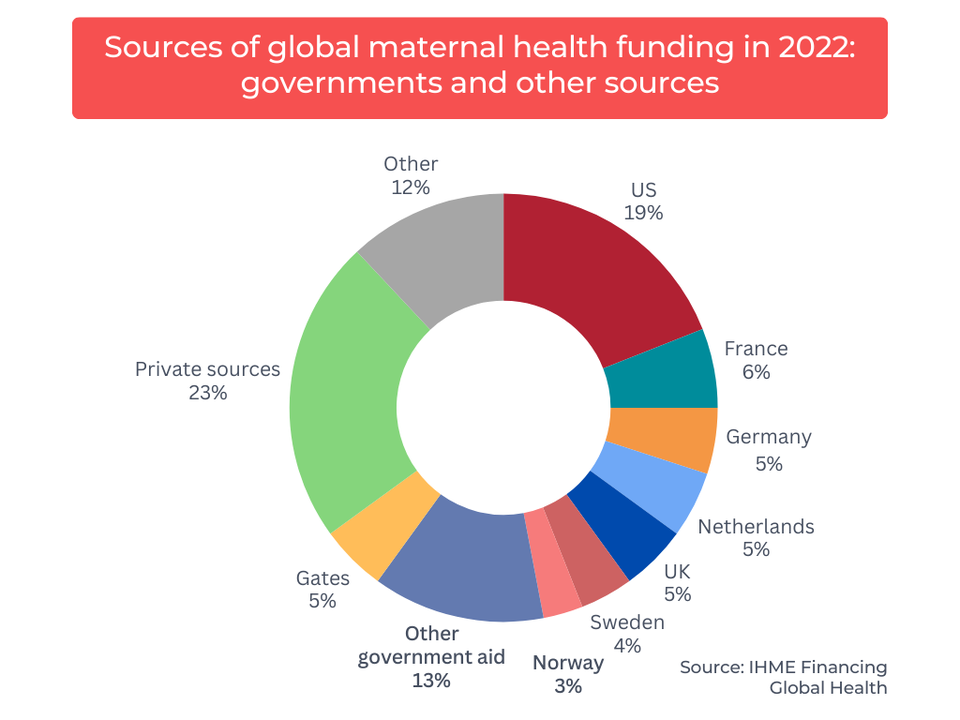
In 2022, funding for global maternal health came from a broad and evenly spread coalition of donors. Source: Analysis of IHME Financing Global Health Data, University of Washington (Accessed March 4, 2025)
1 of 2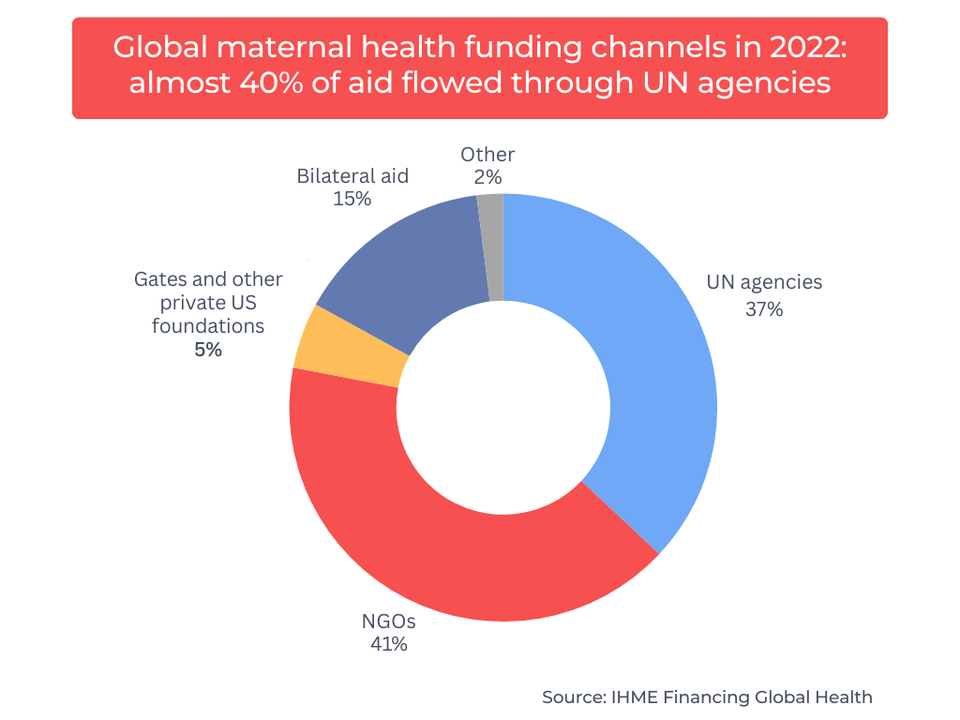
Over a third of global funding for maternal health flowed from donors to recipients via UN agencies, with NGOs another key channel of delivery. Source: Analysis of IHME Financing Global Health Data, University of Washington (Accessed March 4, 2025)
2 of 2Maternal health programs funded by DAH tackle a major cause of global mortality by assisting women in having safer pregnancies and deliveries, including care before, during, and after labor, prevention and treatment of pregnancy-related complications, and routine and lifesaving medications. In 2022, just over half of this DAH went directly to these types of maternal health services. A quarter was invested in health system strengthening, which includes improving health infrastructure and building resilient supply chains, to ensure facilities and lifesaving interventions, like oxygen to support babies in their first breaths, are readily available for safer deliveries.
The remaining quarter of DAH funding was used to support the employment, retention, and training of a skilled health workforce. These investments in human resources for health are vital, as having a skilled health care worker present during childbirth significantly increases the chances of a safe delivery for both the mother and her baby.

Over half of global maternal funding went to direct programming, such as care before, during, and after birth; managing complications; and nutrition. Source: Analysis of IHME Financing Global Health Data, University of Washington (Accessed March 4, 2025)
In April of 2025, the WHO reported that the reductions in DAH have caused significant service disruptions—nearly severe as what countries experienced during the height of the COVID-19 pandemic—with maternal, newborn, and child health among the most severely affected services and community health workers (CHW) and midwives among the most impacted occupations.
We know maternal health service disruptions have life-threatening consequences. An estimated 40,000 additional women died due to pregnancy complications or childbirth in 2021 as a result of the direct complications of COVID-19 and the service disruptions caused by the pandemic.
With many countries experiencing pandemic-level disruptions caused by the diminished financial landscape, it is all the more urgent to find solutions. If other funding sources do not replace these gaps, it’s estimated that between 2025 and 2040, the maternal mortality ratio could increase by 29 percent, with 510,000 additional maternal deaths caused by a lack of available health care services.
Fortunately, there has been some positive news for maternal and newborn health funding. In April, a collective of private philanthropies, including organizations like the Gates Foundation, the Children’s Investment Fund Foundation, and the Mohamed Bin Zayed Foundation for Humanity, launched the Beginnings Fund, committing $500 million to improve maternal and newborn survival in sub-Saharan Africa.
While domestic resources and private philanthropy alone cannot fill all the gaps created by government donors, strategic investments like those from the Beginnings Fund to support a skilled health care workforce and cost-effective interventions can help maintain progress in maternal health.
The current workforce disruption affecting midwives and CHWs could also present an opportunity for other existing donors looking to provide additional support. Our analysis found that more than 70 percent of all maternal health DAH for human resources for health came from smaller government donors, private funders, and other sources in 2022. Modest increases from this group of existing donors, designed with greater input from the countries they aim to support, could help protect access to care in the short term while governments work on the long-term budget and policy changes needed to sustain self-financed health systems.
Modest investments, big impact
Most maternal deaths in low- and lower-middle-income countries are preventable. Moms continue to face life-threatening complications not because solutions don’t exist, but because they lack access to the skilled care and high-quality interventions precisely when they need them the most.
Despite being a relatively modest portion of all global health funding, investments in maternal health have a tremendous impact on the lives of millions of mothers and their infants. While large-scale impact data from leading international development institutions can be hard to come by—often to their detriment as improvements in transparency have been shown to boost citizen support for foreign assistance—both USAID and key UN agencies consistently published impact data for their investments in maternal and newborn health. We analyzed this data to show how many moms and kids were reached and to put those numbers into perspective, highlighting the scale of these programs' impact relative to overall need.
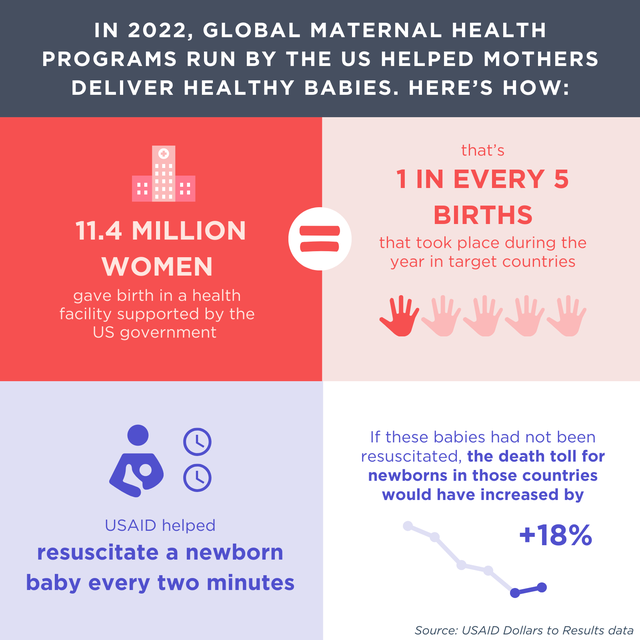
In 2022, bilateral US-run global maternal health programs through USAID helped mothers deliver in health facilities and helped babies take their first breaths. Source: USAID Dollars to Results database, accessed January 2025; UNICEF data on 2022 births.
1 of 5
Analysis sources: USAID Dollars to Results database, accessed January 2025; UNICEF data on 2022 births.
2 of 5
Analysis sources: 2022 annual report of UNFPA's Maternal and Newborn Health Fund, accessed May 2025; UNICEF data on 2022 births; complication rate from Aftab et al, PloS Med 2021: https://doi.org/10.1371/journal.pmed.1003644
3 of 5
Analysis sources: UNICEF 2022 Global Annual Results Report, Goal Area 1; 2022 annual report of UNFPA's Maternal and Newborn Health Fund; and 2021 State of the World's Midwifery report, UNFPA (estimate of number of worldwide widwives). Accessed May 2025.
4 of 5
Analysis sources: UNICEF 2022 Global Annual Results Report, Goal Area 1; 2022 annual report of UNFPA's Maternal and Newborn Health Fund; UNICEF data on 2022 births.
5 of 5Beyond the millions of lives supported with lifesaving care, these investments are financially strategic. In 2022, a UN report estimated that every dollar invested in ending preventable maternal deaths (including meeting unmet family planning needs) returns $8.40 in economic, health, and societal benefits.
This would suggest that the $1.88 billion in DAH provided to UN agencies in 2022 for maternal health could yield more than $15.81 billion in economic benefits.
Driving progress while budgets constrict
While the funding cuts we’re seeing in 2025 have been unprecedented, it’s important to recognize that funding for maternal health has been declining for years. In 2019, the UN estimated it would take $115.5 billion to end nearly all preventable maternal deaths during pregnancy and childbirth, $103.6 billion of which would need to come from new investments. Putting that estimated need at roughly $11.5 billion annually, the DAH for maternal health didn’t even reach half of that in 2022.
Countries can safeguard some maternal health progress, even as they navigate difficult budget decisions, by prioritizing access to lifesaving interventions and bundling services to improve the quality of care. Although scaling up coverage of proven interventions and tools that deliver a high impact for maternal health at a low cost has been slow and uneven, the impact of these interventions is clear.
For instance, Ethiopia reduced its maternal mortality rate by more than six percent every year between 2000 and 2020, significantly outpacing the global average annual decline of 2.2 percent. This success is due in part to the government’s focus on expanding access to essential maternal health commodities. More than 21,000 of the estimated lives saved during this period are attributed to accessing proven maternal health interventions, such as drugs to prevent or treat infections, high blood pressure, and excessive bleeding during and after childbirth, which is the leading cause of maternal mortality worldwide.
These low-cost, high-impact interventions should be bundled where it makes sense to maximize cost efficiency, health impact, and reach. Policymakers can group one-off interventions into evidence-based, context-specific bundles to target the most common causes of death and illness for mothers and newborns.
A trial conducted in 2023 showed that bundling approaches like measuring blood loss with WHO-recommended treatments for postpartum hemorrhage have been proven to reduce severe bleeding by 60 percent, lower the rate of blood transfusions, and decrease incidences of maternal deaths.
Countries lead the way forward
As the dust settles, we’re beginning to see a clearer picture of how countries are responding to budget shortfalls and where the challenges may persist. On the sidelines of the World Health Assembly (WHA) held in May 2025, Ministers of Health and other high-level government officials shared how their governments are responding to the cuts.
For example, in Malawi, the government is developing a domestic health financing strategy through 2030, pursuing private sector partnerships, and integrating essential care services to bring care closer to the citizens. In Kenya, the government is focused on integrating siloed health issues into the existing social health program and exploring public-private partnerships within the country’s central and commercial banks to protect the security of the medicines supply chain and to ensure facilities can use funds from social insurance programs at the facility level.
At another event, a ministry of health representative from Ethiopia noted that Ethiopia is continuing to prioritize preserving access to lifesaving commodities in the wake of funding cuts. However, as the government considers the difficult choices of where to invest with heavy constraints on domestic resources, he also noted that investments in health system strengthening were likely to be cut.
Difficult tradeoffs are to be expected in today’s landscape. Domestic resources alone cannot fill the gaps left by shrinking DAH, and policy change will have a limited impact if the funding gaps make existing challenges in insufficient infrastructure or a shortage of health care workers worse. The Global Financing Facility for Women, Children, and Adolescents (GFF) has a strong track record of mobilizing funds for health systems strengthening, leveraging the $2 billion committed to the partnership into $32 billion dedicated to the health of women, children, and adolescents over eight years.
Right now, the GFF is collaborating with countries to assess the scale of disruption and is considering the evolving landscape in formulating its strategy for 2026–2030, so it may be well positioned to help the countries most impacted by cuts fill that gaps that domestic resources alone cannot cover, using both traditional and innovative financing approaches, as long as it remains relatively protected from the ongoing budget cuts impacting the sector.
For any questions about the methodology and/or data sources used in the analyses throughout this article, please contact advocacyandpolicy@path.org.
*Endnote on our approach: While there is some overlap between funding for maternal and newborn health, and the investments in maternal health are essential to newborn health, this article focused only on maternal health funding. This is because IHME’s data generally combine newborn health investments with child health, which we will explore in a future article.


