
Kendu Bay Sub-County Hospital Vaccines and Immunization Coordinator, Victorine Wasonga (right), speaks with Jane Awuor and her child, Shirley Marion, about the importance of timely childhood vaccination against life-threatening diseases. Photo: PATH
This is the first article in our series exploring what the foreign assistance funding gaps could mean for women and children around the world. Read the second article here and the third article here.
On the shores of Lake Victoria in Kenya’s Homa Bay County, a community-driven immunization program is a testament to the positive impact of foreign investment in global health. With financial support provided by the United States, PATH supported the local government and community health workers in taking innovative approaches to improve vaccination rates among children living in hard-to-reach migrant fishing communities. In just two years, Chuowe Dispensary helped immunization rates in the village jump by 20 percentage points, reaching nearly 90 percent coverage in 2024.
However, in 2025, the progress made in these communities hangs in the balance as the global health landscape undergoes a seismic shift. Many donor countries, including Germany, the Netherlands, France, and the United Kingdom, have been reducing their investment in foreign assistance in recent years—and in January, the United States joined them, rapidly shrinking its foreign assistance footprint as the government overhauls its approach to foreign policy.
As countries, funders, and the private sector face difficult choices as they consider what to prioritize in the months and years to come, a cross-cutting question requires urgent attention: what does this mean for the health of women and children?
Maternal, newborn, and child health is foundational to achieving health equity
Maternal, newborn, and child health (MNCH) services have been one of global health’s best investments for decades. They help women live healthier lives, give children a stronger start to grow up healthy and thrive, and generate tremendous economic benefits.
Investments in MNCH have an incredible impact. Since 2000, highly effective and low-cost solutions have helped cut preventable maternal deaths by nearly 40 percent and child deaths by more than half, helping more kids than ever before reach their fifth birthdays. These foundational investments have played a crucial role in building strong and resilient health systems that expand access to lifesaving care for those with the greatest need. Around the world, MNCH programming is often the first—and sometimes only—touchpoint that people have with primary health care services.
Given the foundational role MNCH plays in building stronger, more resilient health systems and communities, we undertook this analysis to look at the funding gap for MNCH and its impact. The following questions guided our analysis:
- What is the estimated portion of global foreign assistance allocated to MNCH assistance programming?
- Within that MNCH assistance programming, what kinds of activities were funded?
- How exactly did it change lives? And how might its absence affect people in the future?
- Where will the impact of reduced foreign assistance be felt most acutely?
This will be the first in a series of articles digging into the size, nature, and impact of the global funding gap for MNCH. As this landscape continues to evolve, the available data is imperfect and may evolve in turn, but these questions and this moment require urgent consideration.
Leveraging financing data from the Institute for Health Metrics and Evaluation (IHME), impact data from USAID’s Dollars to Results database, and direct stories from PATH experts and our partners around the world, we will share a preliminary analysis of what the data suggests about these essential questions and the impact of investment in these programs. We will also share where low- and middle-income countries are filling gaps and what opportunities exist for stakeholders interested in helping protect some of the progress that remains at risk.
Global investments and the scale of the impact on maternal, newborn, and child health
To begin answering those core questions, we began by reviewing the scale of global foreign aid for MNCH. We analyzed IHME’s Financing Global Health data on how much foreign assistance global donors provided for MNCH, including immunization, nutrition, and malaria treatment and prevention.

This infographic details the total amount of DAH funding provided by all global donors for maternal health, newborn and child health, and malaria in 2022.
In 2022—the most recent year for which we have both impact and funding data—global donors mobilized $17.81 billion in development assistance for health (DAH) for MNCH. Over half of this funding ($9.53 billion) went to newborn and child health, including immunization and nutrition, followed by slightly less than a third ($5.05 billion) for maternal health, and about a sixth ($3.23 billion) for malaria. Much of the malaria funding comes from the United States.
The three largest government donors—the US, the UK, and Germany, which have all announced significant cuts to their DAH in 2025 and beyond—make up a third of all DAH for MNCH, followed closely by private funders, which provide almost a quarter, and the Gates Foundation, which provided 10 percent.
While a significantly reduced investment in foreign assistance will have critical impacts on a broad ecosystem of actors—including large multilateral institutions like United Nations agencies and the World Health Organization, as well as nongovernmental organizations—nearly 40 percent of all DAH for MNCH in 2022 was delivered directly from one government to another. Globally, 126 countries received aid funding for MNCH in 2022, three-quarters of which went to sub-Saharan Africa.
In particular, the Democratic Republic of the Congo, Nigeria, Bangladesh, Tanzania, Ethiopia, Mozambique, and Uganda were the top recipients of DAH funding for MNCH. Countries that rely significantly on external funding face the challenge of rapidly mobilizing additional domestic resources for health if they are to protect access to MNCH care and safeguard decades of hard-won progress in health outcomes. While this may be feasible for some middle-income countries, for many low-income countries, and especially those experiencing conflict or fragile health systems, domestic resources alone cannot meet all of the population’s health needs. Without strategic intervention to fill the gaps left by donor governments and continued solidarity in pursuit of ambitious global health goals, the impact of funding cuts may soon be measured in lives lost around the world.

The US, UK, Sweden, Netherlands, Germany, and France—responsible for nearly 43% of all DAH for MNCH in 2022—have all recently announced cuts to foreign assistance, likely to result in significant funding challenges for lifesaving MNCH services worldwide.
1 of 3
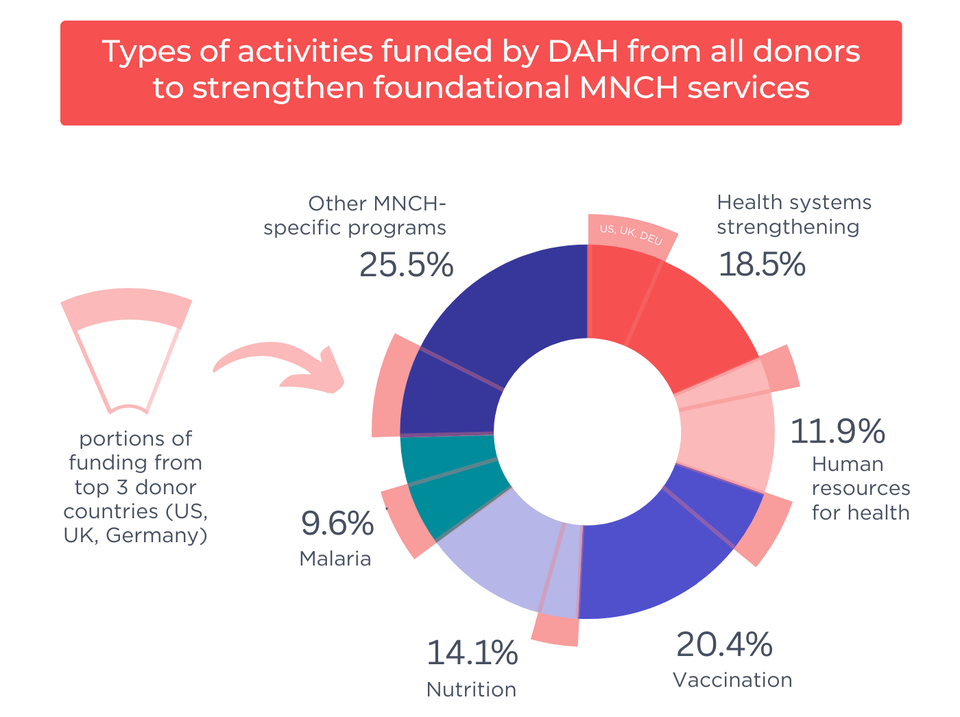
This infographic shows how the top three donors prioritize their investments across health areas.
2 of 3
This chart shows which regions received the most DAH support for MNCH, by volume. The vast majority of funding went to sub-Saharan Africa, South and East Asia, and the Pacific.
3 of 3The human impact of investment
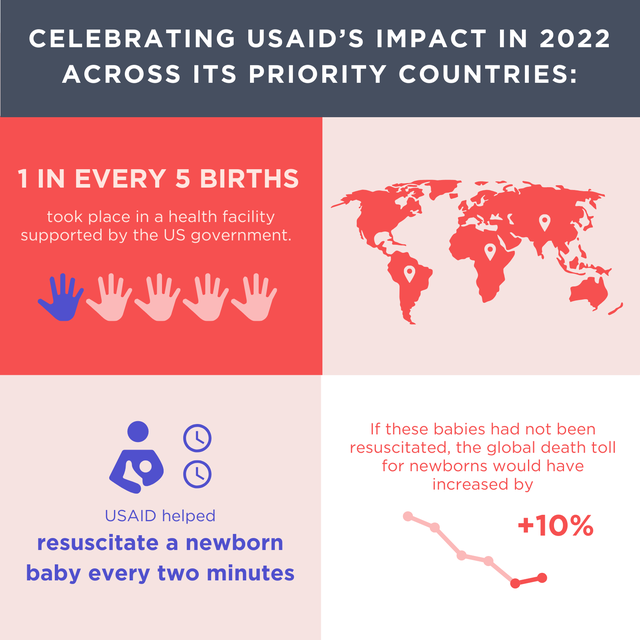
Behind the billions of DAH dollars mobilized every year are real lives positively impacted. More children than ever before are living to celebrate their fifth birthday and since 2000, the maternal mortality rate has decreased by more than 33 percent.
This is remarkable progress, and we can reasonably assume it was possible partly due to more than three decades of sustained DAH investments from donor countries. Progress began accelerating roughly around the same time that global donors stepped up efforts to prioritize child survival in the 1990s. Unfortunately, only the United States was consistently transparent in communicating how taxpayer dollars reached mothers and children around the world.
In 2022, the US spent $3.1 billion, more than $1.6 billion channeled through USAID alone. Leveraging USAID’s Dollars to Results data, we can begin to bring to life the impact that US DAH for MNCH had around the world, primarily in sub-Saharan Africa and South Asia.
 1 of 3
1 of 3
 2 of 3
2 of 3
 3 of 3
3 of 3
Cracks in the foundation of health systems
The size of the overall funding gap or the number of people reached by specific treatments is not the only concern. Though MNCH may seem like a relatively narrow focus, the funding gap to MNCH could lead to a massive crack in the foundation, undermining the resilience of essential health systems if resources are not swiftly mobilized to replace vital DAH funds.
Our analysis shows that in addition to supporting specific disease and treatment portfolios, global DAH for MNCH and malaria also supported the foundational tools to strengthen health systems necessary to deliver lifesaving care effectively: hiring and training health care workers, including skilled community health workers essential to reaching the hardest-to-reach; strengthening delivery systems and supply chains to ensure all communities can access the lifesaving medicines they need; and improving disease surveillance to help stop the spread of infectious diseases.
Across all donors, 30 percent of all DAH funding for MNCH were investments in health systems strengthening (HSS) and human resources for health. For the top three government donors in this space, while prioritization of specific interventions varies—for example, the US was more focused on malaria diagnosis and treatment, whereas the UK and Germany favored investments in vaccines and, in Germany’s case, nutrition—around $1 of every $5 spent went to HSS and about $1 in $10 went to supporting the workforce.
Nearly two-thirds of DAH for MNCH given in 2022 went to foundational activities, such as health systems strengthening, workforce support, nutrition, and vaccination, that underpin capable and resilient health systems.
1 of 2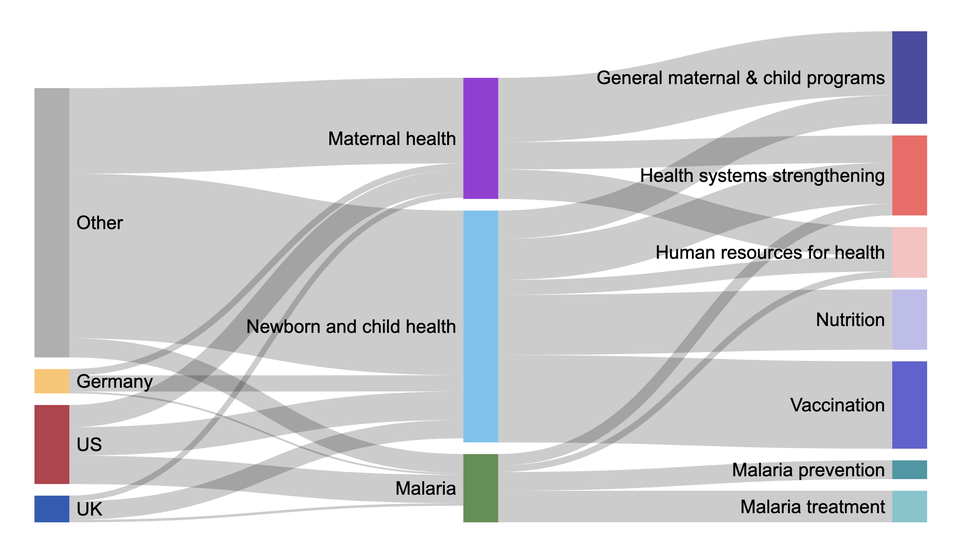
This chart shows funding flows from the three largest donors (and other sources) to health areas of maternal, newborn, and child health, split out by different activities.
2 of 2Private funders may be best suited to fill these systems gaps quickly, at least in the near term, as countries make difficult budget decisions to reflect significantly diminished funds from donor governments. In 2022, private funders surpassed all other donors for human resources for health, supplying nearly one-third of all funding for a more robust MNCH workforce, and were among the top donors for stronger MNCH health systems at more than 16 percent.
Looking forward, diving deeper
As the foreign assistance landscape is changing rapidly, it will be critical that donors and recipient countries work together to mitigate risks and sustain the wins and systems that have been built of over decades. Understanding how these investments work together and the existing gaps should help drive conversations about the future of foreign aid.
Over the coming weeks, we’ll continue our analysis of the impact of funding cuts on core MNCH programming, nutrition, immunization, and malaria in greater depth and make recommendations specific to those funding areas on how to best move forward and protect decades of progress of improving women’s and children’s health around the world.
Endnotes
- PATH accessed and downloaded the USAID Dollars to Results dataset from the agency’s website in September 2024. An archived version can be accessed through the Internet Archive’s Wayback Machine initiative.
- Institute for Health Metrics and Evaluation (IHME). Financing Global Health. Seattle, WA: IHME, University of Washington, 2024. Available from http://vizhub.healthdata.org/fgh/. (Accessed March 4, 2025.)
- While not always discussed as an MNCH investment, malaria has an outsized impact on MNCH outcomes, with children under five and pregnant women making up nearly 80 percent of the estimated 597,000 malaria deaths in 2023. It is because of this significant overlap that malaria is included in this analysis.


